Types of Nipple Discharge
Nipple discharge is the production of fluid from the nipple. The fluid comes from the milk gland ducts that open at the nipple. Most cases of nipple discharge are due to normal, benign conditions and are usually hormone-related. Approximately one third of all women can produce a nipple discharge by gently massaging their breasts. This ‘innocent’ nipple discharge usually comes from multiple ducts in both breasts in pre-menopausal women. Bloodstained discharge from a single duct in one breast can be sinister in nature and may represent an underlying carcinoma.
What Do I Do if I Have Nipple Discharge?

Women with nipple discharge should consult their family doctor without delay. They may then be referred to a breast specialist who will examine the breasts in more detail. Depending on the number of discharging ducts and the colour of the discharge produced, the specialist may arrange further investigations including microscopic examination of the discharge fluid, an ultrasound scan (if the patient is younger than 35 years) and/or a mammogram (if the patient is older than 35 years).
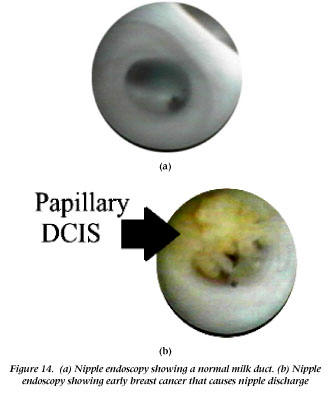
Occasionally a breast lump is found in a patient presenting with nipple discharge. Such lumps are investigated appropriately. If the microscopic examination and mammography/ultrasound show no worrying features, the patient can then be reassured. Women with blood-stained discharge coming from a single milk gland duct, and showing abnormalities on microscopic examination, will require surgical excision of the discharging duct. The operation to removing a single duct is known as a microdochectomy and is usually performed as a day-case. The removed tissue is sent to the pathology laboratory for further examination. In some centres it is also possible to carry out a camera examination of the nipple duct, which is called mammary ductoscopy. The author has recently introduced this new technology into his practice (Image below).
Clear discharge arising from multiple milk gland ducts is usually normal. It does not require treatment unless it becomes troublesome or associated with abnormal microscopy or mammography, when surgery may be considered. The operation consists of the total removal of all the ducts draining into the nipple. The main risks of the procedure include the death of the nipple tissue (uncommon) and the reduced sensitivity of the nipple area (in one third of cases). Such complications should be weighed against the severity and inconvenience of the symptoms.
What Does a Milky Discharge Mean?
Milky discharge through the nipple, called galactorrhoea, is normal during and within 2 years after pregnancy. Milky discharge occurring outside pregnancy can be caused by an imbalance of the hormone prolactin, which controls milk production. A small gland in the brain called the pituitary gland produces prolactin. Tumours arising in this gland may cause excessive amounts of prolactin to be released into the bloodstream, thus stimulating the breast tissue to release a milky discharge. A brain scan may be required to look for tumours in the pituitary gland. Pituitary tumours are usually benign and are easily treated with drugs or by surgery. If prolactin levels are within normal limits, the patient can be reassured that the discharge is likely to improve without further intervention.
Other Causes of Nipple Discharge
| Inflammation and dilatation of the nipple duct | Benign tumour of the nipple duct | Breast cancer |
| Called periductal mastitis/duct ectasia Pain and nipple inversion are common More common in smokers Improved by stopping smoking and by antibiotics Surgery if persistent |
Called intraductal papilloma Single-duct blood-stained discharge Treated by surgical removal No follow-up is required |
Non-invasive (DCIS) type Does not usually spread Mastectomy is required as it is close to the nipple Surgical treatment is curative (98%) |


For more information on papillomas from articles written by Professor K Mokbel
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1524964/ and https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1395317/
