Benign Breast Lumps
The majority (80%) of breast lumps detected are benign, i.e. are not cancerous. Benign breast lumps represent alterations in normal breast development; they are essentially harmless and often disappear with time. Sometimes, however, they can be difficult to distinguish from a malignant (cancerous) lump and an incorrect diagnosis can have serious consequences.
Fibroadenoma (Breast ‘Mouse’)
A fibroadenoma usually appears as a well-defined, firm lump in the breast. They are often very mobile, hence the name breast ‘mouse’. These benign lumps represent an alteration in the normal development of the breast and are dependent on the sex hormone oestrogen. Fibroadenomas can occur as a single lump, as multiple lumps, and can even occur in both breasts. They can grow rapidly, especially in adolescent girls, and if they reach a size greater than 5 cm in diameter they are known as giant fibroadenomas.
Fibroadenomas can occur at any age but are most commonly found in younger women, usually between 15 and 30 years of age. They are also seen more often in African women than Caucasians.
If you are aged 15–30 years and discover a well-defined, smooth, firm and mobile lump in your breast, the most likely diagnosis will be fibroadenoma. However, you must see your family doctor, who should refer you to a breast specialist. The specialist will examine the breasts, arrange a mammogram and/or an ultrasound scan of the breast and perform a needle biopsy to confirm the diagnosis.
Once the diagnosis has been confirmed, the specialist will offer you the option of having the lump removed under general or local anaesthesia or being followed-up in the clinic once more in 6 months’ time. If there is any doubt regarding the diagnosis, then a larger biopsy (core biopsy) or removal of the lump will be recommended.


What Happens if I Have a Fibroadenoma?
If the three tests (physical examination, ultrasound scan and/or mammogram, and needle biopsy) confirm the diagnosis of fibroadenoma, then you may find yourself in a dilemma regarding what to do about it. Studies have shown that one in four fibroadenomas shrinks or disappears completely within two years of diagnosis, about one in two stays the same size, and only around 25 in every 100 actually get bigger.
For women under the age of 30 years, the best option is to leave the lump alone and have a follow-up assessment (via ultrasound scan) in 6 months’ time. Provided the diagnosis is confidently made with needle biopsy and ultrasound scan and the lump has not grown larger after this time, the patient can be reassured and discharged from the clinic. Women with a strong family history of breast cancer may be advised to have any breast lump removed. For women aged over 30 years, the lump can be left alone if the diagnosis is confirmed with ultrasound-guided core biopsy. Alternatively the lump can be removed surgically. This is a relatively minor operation that is usually performed as a day case through a cut around the nipple. It can even be done under a local anaesthetic. There is usually minimal breast distortion and scarring and does not increase your chance of developing breast cancer.
Surgical removal will avoid missing the occasional breast cancer that may occur, although the chance of having breast cancer here is very small. Innocent lumps like fibroadenomas can be also removed through key-hole surgery using a vacuum-assisted device under local anaesthesia in the clinic. This facility requires expertise and is not widely available. If the patient is not keen on having open or key-hole breast surgery, an ultrasound scan can be performed in 6 months’ time in order to monitor the lump’s size and provide further reassurance.
Patients with lumps larger than 3 cm are advised to have the lump surgically removed, especially if they are over 40 years of age. This is because, in some cases, it can be extremely difficult to distinguish between fibroadenoma and a type of breast tumour called a phyllodes tumour. However, there is no evidence to suggest that breast cancer develops from fibroadenomas.
In the author’s opinion, if the diagnosis of a simple fibroadenoma is confirmed with ultrasound-guided core biopsy then it can be safely left alone if it is smaller than 3 cm in size. The key-hole approach using a tiny scar ( 2mm ) should be used if the patient requests removal of a fibroadenoma smaller than 3 cm.
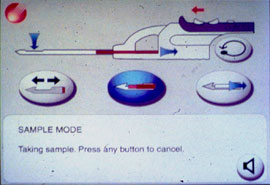
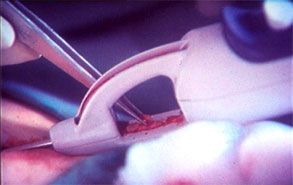
The Principle of key-hole removal of benign breast lumps
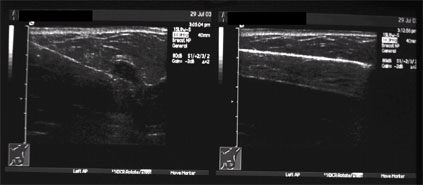
The fibroadenoma seems to have disappeared after removal by the key-hole approach (ultrasound images)
Phyllodes Tumour
This is a rare cause of breast lumps. The tumour resembles a fibroadenoma (breast mouse) but tends to occur in older women (of 35–50 years). Phyllodes tumours can be benign, borderline malignant or frankly malignant (cancerous). Benign phyllodes tumours are more frequent than either the borderline or malignant types.
Phyllodes tumour is treated by surgical removal of the lump together with a rim of the surrounding normal breast tissue. This is called a wide local excision. The lymph glands in the armpit are not usually removed for this tumour. An interesting feature of phyllodes tumour however is the fact that it may recur even if it is benign and has been removed surgically. Overall, the chances of this rare tumour spreading to other parts of the body are very small indeed, and patients with this condition can be reassured and followed up in the breast clinic with yearly visits. Neither radiotherapy nor chemotherapy plays a significant role in the management phyllodes tumours.
