Approximately 1 in 5 patients with breast cancer will require a mastectomy rather than a lumpectomy. As mastectomy results in the distortion of the body image, it is natural for some patients to seek reconstructive surgery. However, some women are just relieved to have had the cancer removed and are not keen on having breast reconstruction. Although an external implant is available that can be put inside the brassiere, it may be adequate for some women. Other women will require surgical breast reconstruction to give them a satisfactory appearance. All patients undergoing mastectomy should be offered the possibility of breast reconstruction, either performed immediately at the time of mastectomy, or as a later procedure. Mastectomy combined with immediate reconstruction is preferred and seems to cost less than mastectomy with subsequent delayed reconstruction. There is no evidence that immediate reconstruction at the time of mastectomy worsens the breast cancer outlook. Frail patients with other medical problems are not advised to undergo breast reconstruction surgery as they have an increased risk of complications.
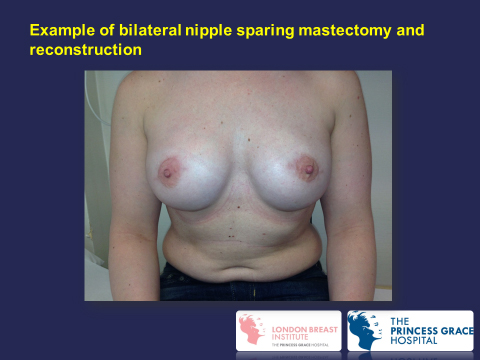
There are various methods of reconstruction and the choice should be made after discussion with the breast surgeon, specialist breast nurse and other patients who have had breast reconstruction. You should request to see pictures showing the outcome of the various methods. The choice of reconstruction depends upon the woman’s build, shape and size of her breasts, previous scars, and her own preferences. I prefers the type of mastectomy that preserves most of/or all the natural skin envelope of the breast (called a skin-sparing mastectomy) when performing immediate breast reconstruction in view of the superior cosmetic result. In selected cases the nipple can be preserved during skin-saving mastectomy and reconstruction in order to achieve a superior cosmetic result (nipple-sparing mastectomy). The various methods of replacing the breast volume during reconstruction include:
- Breast implants (saline-filled tissue expanders or silicone implants)
- Flaps (from back: LD flap, tummy: free DIEP or buttocks free GAP)
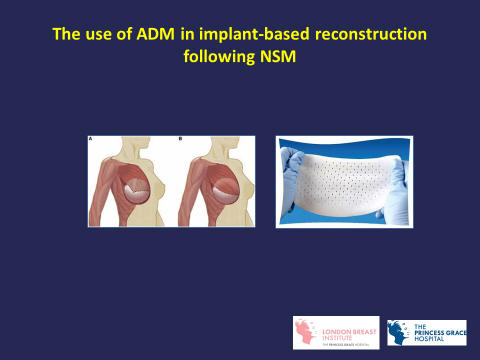
Implant-based reconstruction
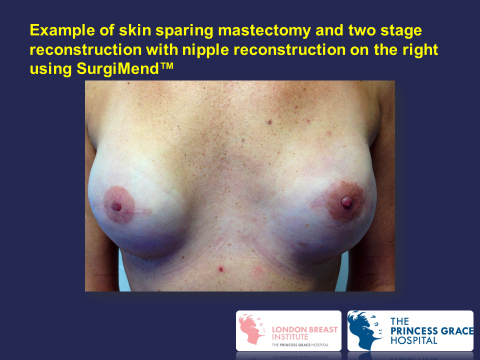
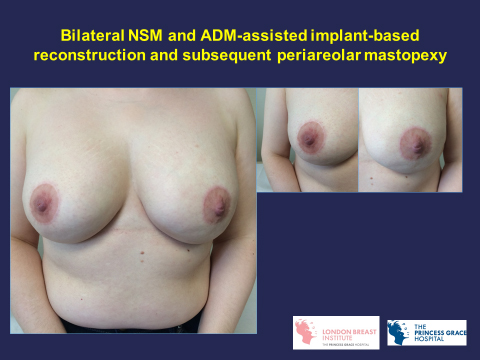
An implant is inserted under the pectoral muscle (sub-pectoral) or in front of the muscle (pre-pectoral) in the chest following mastectomy. Implant reconstruction can be performed immediately at the time of skin-sparing mastectomy or as a delayed procedure through the original mastectomy scar. A biological mesh derived from animal tissue call acellular dermal matrix (ADM) is now routinely used during immediate reconstruction following skin-sparing mastectomy to cover the lower pole of the implant in sub-pectoral reconstruction or the whole implant during pre-pectoral reconstruction. The main problems with implants are infection (occurring in 2% of patients) and scarring around the implant (called capsular contracture) causing hardening and sometimes pain. Scarring can make the breast feel hard and painful, and it is more common if the prosthesis is very smooth and if a mesh is not used. A rare form of cancer that can develop in the scarring tissue around the implants called anaplastic large cell lymphoma (ALCL) has been recently described. It incidence is estimated to be 1 in 30,000 and is more likely to occur with textured rather than smooth implants. However smooth implants have higher risk of capsular contracture (double the risk) compared with textured implants and on balance the latter is still the preferred option.
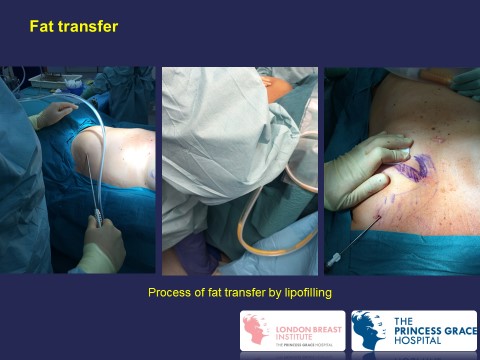
Fat transfer has been recently used to complement implant-based breast reconstruction.
Most modern implants contain cohesive silicone gel. Saline-filled implants can be also used. The implants can be round or teardrop shaped (see below).

The LD flap (back) for reconstruction (+/-implants)
The various steps of skin-sparing mastectomy and immediate reconstruction using the LD flap.






The long-term cosmetic result of SSM (right) plus LD flap reconstruction 13 years ago
Nipple Reconstruction
It is also possible to reconstruct the nipple using local skin, a portion form the opposite nipple, or a skin graft taken from the groin. The new nipple can be tattooed to make it a similar to that of the opposite nipple. A disposable tattooing instrument is used to minimise the risk of disease transmission.
The steps of performing nipple reconstruction using a small local flap:


Fat transfer to complement breast reconstruction


For information on ALCL click here
For more information on nipple sparing mastectomy from articles written by Professor K. Mokbel
https://www.ncbi.nlm.nih.gov/pubmed/27462565/
For more information on fat transfer to the breast from articles by professor Kefah Mokbel
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4366692/
‹‹Previous Reconstruction Continued…››
